| T
H E N I H C A T A L
Y S T |
J U L Y – A
U G U S T 2003 |
|
SARS
Coronavirus Could Resurface in Chilly Weather
PROPOSED
CC/NIAID PROTOCOL AIMED TO
GO
AT FIRST LOCAL RESURGENCE
OF SARS
|
by
Fran Pollner |
 |
| Kathryn Holmes, "SARS-Associated Coronavirus, NEJM
348:
1948-1951, May 15, 2003; shown also during her talk on coronavirus virology
and pathogenesis at the NIH workshop May 30 |
|
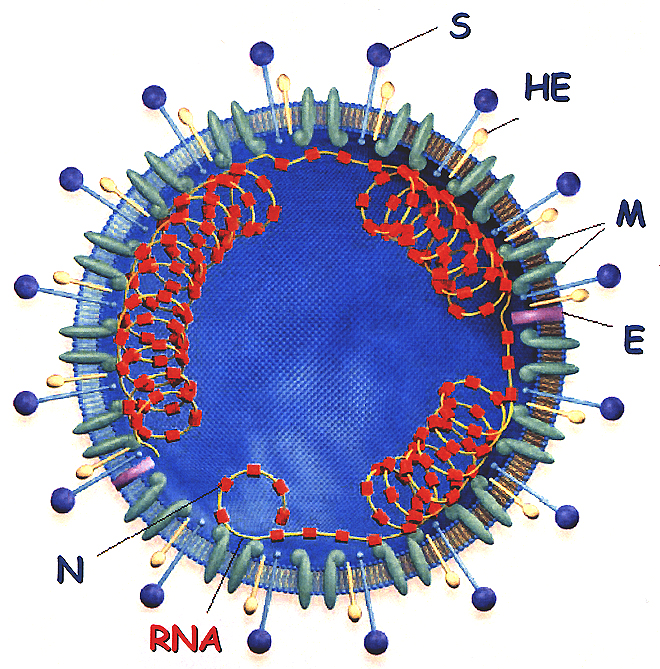
Structure
of the Coronavirus Virion: S = spike glycoprotein (the viral fusion protein),
HE = hemagglutinin-acetylesterase glycoprotein, M = membrane glycoprotein,
E = small envelope glycoprotein, N = nucleocapsid phosphoprotein
|
The
chain of events that led to a World Health Organization warning against traveling
to Toronto began with the hospital spread of SARS from a patient and his wife.
The couple passed the virus to 84 people in 31 hours.
Most of those infected,
said Allison McGeer, director of infection control at Mount Sinai Hospital and
a professor at the University of Toronto, had been "within droplet range
for no more than one to two minutes."
Within days of this event,
which turned out to be a rare example of a SARS "superspreader," 19
Toronto hospitals were affected by SARS, and every one of them wanted to be
able to get a clinical trial going, McGeer recounted during a clinical research
breakout session at the international SARS colloquium
held at NIH May 30.
"But there was no
way they could get a clinical trial protocol through the ethics boards of 19
hospitals before the outbreak, which lasted a month, was over—not to mention
that it’s hard to focus on anything but treating during an outbreak. This
is a major challenge," she said.
Many agreed that new mechanisms
are needed for rapid—but careful—approval of national and international
protocols to respond to such precipitous events.
 |
| Teamwork:
(left to right) Henry
Masur, CC critical care chief and an associate investigator in the CC/NIAID
SARS protocol; John
Beigel, CC clinical research fellow and protocol PI; and Cliff
Lane, NIAID clinical director and the protocol's accountable investigator |
Meeting
the Challenge
Investigators generally
view the next cold-weather flu season as a likely context for SARS resurgence.
Collaborating scientists from NIAID and the CC are seeking IRB approval of a
SARS clinical research protocol that would begin the instant the first patient
in the metropolitan area thought to have SARS is referred to NIH as a study
candidate.
The protocol encompasses
three study cohorts comprising up to 200 individuals: SARS patients, their household
contacts, and CC health-care workers.
"A major issue,"
said Henry Masur, chief
of critical care medicine
at the Clinical Center, "is how the virus is spread, and a major thrust
of the study is determining from where, how much, and for how long the virus
is excreted."
The protocol targets patients
who have relatively mild disease when they are invited to enroll. It’s
anticipated that most of the patients would drive themselves to the Bethesda
campus and be met at the perimeter and transferred via a dedicated negative-flow
transport device (see photo below). They wouldl enter the hospital through a
special entrance and be taken directly to a negative-flow room.
Blood, urine, feces, and
respiratory secretions would be analyzed on a regular basis. Among the study
goals listed in the protocol are:
 To evaluate and treat persons with SARS
To evaluate and treat persons with SARS
 |
Private
Spaces:
The DeMistifier rolling bed/isolation unit, acquired to transport a SARS
protocol patient from his or her vehicle to a secure CC entrance and up
to the negative-flow room where the patient would be cared for—with
CC respiratory
therapy chief Dennis
Brown in attendance, as would often be the case throughout the upcoming
study. Brown is wearing the powered air-purifying respirator (PAPR) and
protective gown, gloves, and foot gear that all involved health-care workers
would don while participating in the study. Filtered air is delivered
to the hood by tube from a pack worn around the waist; the hood is disposable
and after each patient encounter would be discarded in the anteroom outside
the negative-flow room. Brown says he is not too worried about his personal
safety: "I wouldn’t have signed on as a health-care provider—especially
at NIH—if I didn’t know some risk was involved." Brown
and others, including hospital epidemiologist David
Henderson, believe this risk is minimal based on the ability of hospitals
in Asia and Toronto to control SARS once they understood and enforced
the necessary precautions.
|
To elucidate the pathophysiology of SARS
To characterize the immune response during SARS
To evaluate diagnostic tests for the rapid identification of SARS in clinical
specimens
Contacts:
Household and Hospital
The second study population
of family members and other close contacts would be enrolled and followed serially
for evidence of the onset of viral excretion and correlation with the presence—or
absence—of clinical symptoms. Data generated from this cohort should expand
knowledge of the natural history of the disease. "We’d have an unparalleled
opportunity to study disease development virlogically and immunologically from
very early after exposure."
|
'We announced in April that we might bring
SARS patients to the Clinical Center to participate in a study. We felt
we have a fabulous environment scientifically—and a safe environment—to
study SARS. But that possibility generated more e-mail to me than anything
else in the eight years I’ve been Clinical Center director.'
—John
Gallin
'The facts of the evolution [of the SARS
outbreak] show that when the medical staff is prepared, the chain of transmissibility
is broken. The risk of spread in a hospital that is conducting a study
is low.'
—Anthony
Fauci
CC Grand
Rounds, June 18, 2003
|
The third population—NIH
health-care workers who come in contact with the study patients—would be
followed to "make sure they are not acquiring the virus.
"While the risk of
a hospital worker becoming infected is remote, that possibility does exist,"
Masur said. "Should that happen, the person would be moved into the other
protocol group—but the hospital leadership and NIAID leadership have confidence
in the caliber of our facilities and our staff and our ability to handle this
virus better than can be done almost anywhere else." He noted that hospital
epidemiologist and CC deputy director David
Henderson, an associate investigator in the study, has discussed SARS transmission
with involved hospital authorities in Canada and Asia and has concluded that
the risk at the Clinical Center should be manageable, as has Cliff
Lane, NIAID clinical director and the accountable investigator on the protocol.
The far greater danger
to any hospital staff and to other patients, protocol
leaders
have observed, would be exposure to CC patients and staff who develop SARS through
travel or personal contact and then enter the building for work or for treatment
on protocols not related to SARS.
"Perhaps the most
important lesson learned from the Toronto experience," Henderson said,
"is that health-care workers at the front-line in an epidemic must have
extremely high indices of suspicion for the diagnosis and proper management
of highly contagious diseases such as SARS. Almost all instances of transmission
occurred in settings in which the disease was not suspected." Conversely,
once the disease was recognized, even institutions in developing countries with
limited resources were able to contain the infection by careful adherence to
traditional infection-control procedures.
Aside from CC excellence
in infection control, other factors that argue for clinical SARS research at
the CC are the NIH tradition and responsibility to respond to national health
priorities, protocol investigators agree. They point to the response of the
CC to the AIDS epidemic in the early 1980s, when there was considerable fear
about having patients with HIV in hospital settings, as an example of meeting
that obligation and advancing science and patient care in a perilous time.
Beyond
the First SARS Protocol
The CC/NIAID investigators
also envision two additional studies that could culminate in the development
of a novel SARS therapy. The first would entail identifying patients who have
recovered from SARS and bringing them to the Clinical Center to obtain plasma
samples from them.
"The idea is that
we can use these samples to make an immune serum globulin. We know that SARS
patients make antibody to the virus," Masur said. "We would harvest
that antibody, concentrate it, and remove potentially infectious elements."
This potential product would be tested in a variety of in vitro studies and,
if results warranted and the FDA approved, would then move into human testing.
In the current protocol,
treatment is described in flexible terms:
"As there is no clear
optimal therapy, and the data regarding optimal therapy for SARS [are] continually
changing, two options will be presented to the patients regarding therapy. First,
the patients may be treated as clinically indicated by best medical practice
given our continually changing knowledge of SARS.
"Alternatively, patients
may be enrolled in other protocols designed to evaluate therapies. These may
be intramural protocols of the NIH or protocols from outside study groups for
which the NIH is a collaborative center."
SARS:
IMPACT AND RESPONSE
SWIFT AND W0RLDWIDE |
 |
| Front
and Center: NIAID
Deputy Director John
La Montagne (foreground left) and NIAID Director Anthony
Fauci confer at the start of the SARS research colloquium at NIH
on May 30. The meeting, Fauci said, "was put together as quickly
as SARS has spread." |
A
critical mass of international scientists converged at NIH May 30 to construct
a research agenda to defeat severe acute respiratory syndrome (SARS).
The global scourge had infected 8,439 people and killed 812 by the time
the first recognized outbreak was declared contained a month later.
A global report
from the World Health Organization, first-hand accounts of the Hong Kong
and Toronto outbreaks, and lectures on coronavirus biology set the stage
for five concurrent working groups to hammer out research recommendations
by the end of the day.
This research agenda
was speedily transferred to cyberspace at this
site, which also displays all the slides presented throughout the
day; the plenary talks can also be viewed here.
|
Return to Table of Contents