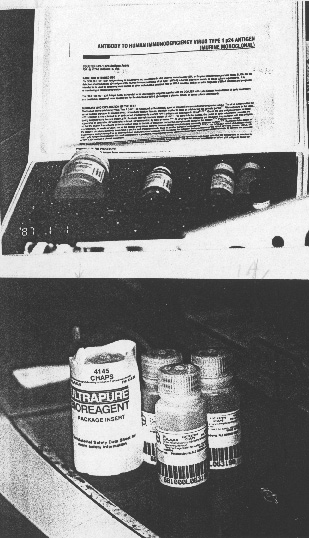
Two
of many standout NIH inventions: an HIV antibody test kit (above) and
CHAPS
| T H E N I H C A T A L Y S T | M A R C H – A P R I L 1997 |
|
|
|
NIH INVENTIONS:FROM THE SUBLIME TO THE UBIQUITOUS |
text
and photos by Fran Pollner |
|
|
Two
of many standout NIH inventions: an HIV antibody test kit (above) and
CHAPS
|
If necessity is the mother of invention, NIH may be the mother of necessity. Some of the most vastly useful—and lucrative—inventions to emerge from NIH research sprang from scientists' need to advance their own research, to take their experiments to the next step. The results of their efforts, naturally enough, were laboratory tools appreciated by scientists the world over.
Thus, the value of an NIH-patented zwitterionic detergent, popularly known as CHAPS, has not diminished since its market debut in 1981. In fact, it's one of a fairly exclusive club of top moneymakers for the Public Health service, defined as a PHS-invented commercialized product that exceeds $100,000 in annual sales. In 1995, 28 inventions fit that category (see "Inventions" chart).
At a price of $48.40 for a 5-g bottle (at the NIH self-service store), CHAPS is clearly not a high-ticket item. But it is a high-volume item. Zwitterionic agents, which bear both positive and negative charges, enable the release of biochemically active proteins from cellular membranes without disrupting the proteins' chemistry, composition, or structure. This makes CHAPS a crucial tool in protein purification.
"It's used in almost every laboratory in the world that does basic biological research," said Maria Freire, director of the NIH Office of Technology Transfer. But, she adds, "I don't think people realize it's an NIH invention."
To stoke the tech transfer fires of the ICD scientific directors, Freire brought a carton of NIH inventions to the directors' year-end meeting a few months ago. "You'd be surprised at how many people looked at the CHAPS bottle and said, 'CHAPS! I didn't know CHAPS was invented at NIH!'"
Some NIH inventors and inventions approach household-name status, like NCI's Robert Gallo and his standout moneymaker: a detection assay for HIV-1 antibodies. Gallo's kit brought in $5.5 million of the $27 million in royalties that NIH received last year and has accounted for $50.7 million of the $122 million total NIH royalties since 1987. But Gallo and his test are the exception. Most inventors—like CHAPS inventor Leonard Hjelmeland, a biochemist no longer at NIH—labor in relative obscurity.
Freire's concern at the moment is not winning fame for NIH inventors but, rather, making sure that nascent NIH inventors are not overlooking the "invention potential" of their research. Recently, the number of invention-disclosure reports has been going down, a worrisome trend, she says, since these reports constitute the pool from which OTT pursues patents and licensing agreements. They serve notice that the researcher and his or her ICD tech-development coordinator think they've got something new; thereport is the first step in the tech-transfer process.
 |
 |
|
Maria
Freire (above) and Steve Ferguson, of the NIH Office of Technology Transfer
|
There were 196 reports in 1996, compared with 271 in 1995, with all institutes showing a decline except NICHD. "We need a bigger pool," Freire says. She notes that although OTT decided a few years ago to file fewer patents than in the past—selecting the patent route for about 60 percent of disclosure reports instead of 90 percent—that shift doesn't mean that discoveries are ignored, only that the transfer mechanism chosen is better tailored to the nature of the discovery.
|
'Without tech transfer, we wouldn't have CHAPS or the AIDS test or so many of the benefits to the public health that come from these discoveries. It's an inherently good thing to do.' —Maria Freire, OTT |
"We were filing too many patents before; and each one costs about $24,000 to file. [Securing] worldwide protection can cost up to $150,000. But we can get things out to the public and make money for NIH and the inventor without patenting," she says, noting that the licensing process sans patenting costs NIH just $5,000 to $6,000. And licensing fees and royalties from sales can accrue with or without a patent. Freire points to the "neurotransmitter antibodies" entry on the "successful commercialized inventions" list as an example of a product that has paid off without patenting (see "Brainchild without Patent Yields Anybody's Antibodies.")
Products used as research tools are typically not the stuff of patents these days. Says Steve Ferguson, an OTT technology licensing specialist, "Generally, we seek patent protection for those inventions requiring a patent for commercialization—therapeutics, diagnostics, vaccines, instrumentation. We'd think long and hard now about spending that kind of money and resources to patent a research tool."
The OTT balance sheet has improved with the implementation of this approach. Overall, technology-transfer activities cost about $16 million a year. 1996 was the first year that a profit was actually generated—about $11 million, considering the $27 million received in royalties.
Freire observes that this income is very small relative to NIH's $12-plus-billion research budget, or even the $1.3 billion intramural research program portion, but the NIH's tech-transfer efforts are worth the trouble. "It's an inherently good thing to do."
Ferguson points out, "Not only does it bring inventions to the bedside, it rewards the scientists, and money is plowed back into the institutes. It incentivizes the system."
Could commercial incentive play too large a role in shaping NIH research, or could a company's forecast of commercial windfall influence a research project's direction?
Freire thinks not. "One thing you learn very early on," she says, "is that it's almost impossible to get a researcher to do what he or she does not want to do—researchwise. It's the researcher, not the company, who identifies the potential value of the research. And the value isn't in terms of money. Money doesn't matter."
But money does figure into NIH-industry collaborations. A licensing agreement may require a company to pay an initial fee for the license, a yearly fee on an active license, and benchmark payments when clinical-trial success or FDA approval has been achieved. "It's mix and match," depending on the nature of the product, says Ferguson, OTT's point person in such negotiations.
If a marketed product actually emerges and generates sales upon which royalties can be assessed, the NIH cut varies depending on how much NIH contributed to its development.
Examples of a "high-rate" product, Ferguson says, are polyclonal antibodies or antisera sold as research reagents—which NIH typically makes and presents to companies as a finished product needing only to be tested, packaged, and distributed. In the case of a monoclonal antibody, in contrast, NIH provides the cell that secretes the antibody, but the company carries out purification and quality-control operations. The NIH cut would be lower in such cases.
But even "high-rate"
returns won't make NIH wealthy: 8 percent is pretty much the pinnacle of NIH
reward. Royalties range from 1 percent to 5 percent for a diagnostic product
and from 3 percent to 8 percent for a therapeutic product, Ferguson says. (Royalties
are dispersed by a formula to NIH and the individual inventors and their ICDs;
see "Divided Royalties.") NIH royalties,
Freire says, "are never crippling to the cost of the product," an
outcome that would run counter to NIH main concern—and NIH Technology
Transfer Act mandate—that taxpayer-supported biomedical discoveries
find their way to the public bedside. ![]()
|
PHS
INVENTIONS
AMASSING >$100,000
IN SALES
IN 1995
|
|
| RESEARCH MATERIALS | |
| NON-DENATURING ZWITTERIONIC DETERGENTS | NICHD |
| RECONSTITUTED BASEMENT MEMBRANE PROTEIN COMPLEX | NIDR |
| NEUROTRANSMITTER ANTIBODIES | NIDCD |
| G-PROTEIN ANTIBODIES | NIDDK |
| HUMAN D-2 DOPAMINE RECEPTOR | NINDS |
| PROCESS OF SITE-SPECIFIC MUTAGENESIS WITHOUT PHENOTYPIC SELECTION | NIEHS |
| SILVER STAINS FOR PROTEIN IN GELS | NIMH |
| METHOD FOR THE SULFURIZATION OF PHOSPHOROUS GROUPS IN COMPOUNDS ("BEAUCAGE AGENT") | FDA |
| POLYACRYLAMIDE GELS | NIMH |
| IL-4 HYBRIDOMA CELL LINE | NCI |
| DIAGNOSTICS | |
| ANTIBODIES AGAINST HUMAN PNEUMOCYSTIS CARINII | CC |
| SEROLOGICAL DETECTION OF ANTIBODIES TO HIV-1 | NCI |
| SEROLOGICAL DETECTION OF ANTIBODIES TO HTLV-1 | NCI |
| erb-2 ONCOGENE RECEPTOR | NCI |
| BREAST CANCER MONOCLONAL ANTIBODIES | NCI |
| SOLUBLE INTERLEUKIN-2 RECEPTOR | NCI |
| RECOMBINANT CYTOCHROME P-450 | NCI |
| SPECIFIC/SENSITIVE DIAGNOSTIC TEST FOR LYME DISEASE | NIAID |
| CELL LINE PRODUCING AIDS ANTIGENS WITHOUT PRODUCING VIRAL PARTICLES | NIAID |
| VACCINES AND THERAPEUTICS | |
| CANCER CHEMOTHERAPEUTIC DRUG, 2-F-Ara-A | NCI |
| ANTISENSE PHOSPHOROTHIOATE NUCLEOTIDES | NCI |
| ISOLATION OF HEPATITIS A VIRUS STRAIN HM-175 | NIAID |
| TREATMENT OF HIV INFECTION WITH ddI | NCI |
| TREATMENT OF HIV INFECTION WITH ddC | NCI |
| TRIMETREXATE AS AN ANTI-PARASITIC AGENT | NCI |
| ADOPTIVE IMMUNOTHERAPY AS A TREATMENT MODALITY IN HUMANS | NCI |
| INSTRUMENTATION AND DEVICES | |
| FLOW-THROUGH BLOOD CENTRIFUGE | NHLBI |
| FECALATOR DEVICE (FECAL PARASITE CONCENTRATORª) | CC |
Source: Office of Technology Transfer